I have had breast implants for ten years. Everything is fine. Do I need to have them replaced?
No. If you are not experiencing problems with your breasts or breast implants, there is no need to remove breast implants at ten years.
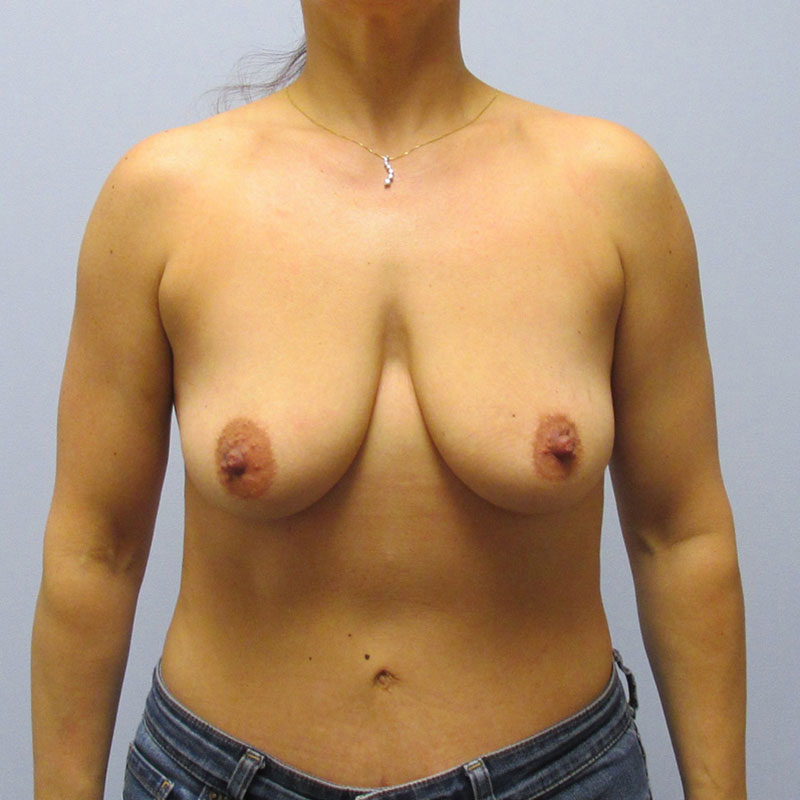
I have had breast implants for many years, have now gained weight, and want them removed. Will I need a breast lift?
You may need a breast lift. Implants over many years will stretch the skin and breast tissue and, when removed, may leave the breasts appearing saggy.
What are the risks of Breast Augmentation?
Bleeding (hematoma formation). Significant bleeding into the space around the implant can occur in this operation, although it is unusual. Large collections of blood around the implant require a return to the operating room for removal. Not doing so would produce an abnormal shape of the breast and a potential for hardening in the future.
Infection. Some of the tissues of the breast normally contain bacteria and are likely to come in contact with the implant during augmentation surgery. All of our patients are placed on antibiotics during surgery and afterward. The risk of infection is less than one percent.
Loss of nipple sensation. Most patients experience some change in nipple sensation following augmentation surgery. The change may either be increased or decreased sensation and lasts several weeks. Nevertheless, the change is usually temporary. Permanent loss of sensation is unusual.
Malposition of implants. Every effort is made to make the breasts appear as symmetrical as possible. This requires fine adjustments in implant placement. On occasion, a second procedure is required to achieve satisfactory symmetry.
There is also a risk of certain long-term complications:
Capsular contracture (hardening of the breasts by the presence of scar compressing the implant). Every individual forms some scar around the implant. This is a normal response of the immune system to a foreign body. For not completely understood reasons, some individuals form thicker scars than others. A thick scar may distort the breast and even cause discomfort. The incidence of this problem is decreased with submuscular implant placement and is approximately ten percent. When treatment is warranted, the scar is incised or removed, and the implant is replaced.
Interference with mammography. Implants interfere with the ability to image the breast by mammography to a variable extent. Implants placed behind the pectoralis muscle allow the breasts to be imaged more effectively by a method called the Eklund Technique. Using this technique, the presence of implants does not represent a statistically significant risk to the patient of missing early breast cancer.
Deflation. The incidence of saline implant leakage is approximately two percent in Dr. Capella’s practice. Today’s implants are better than a decade ago, so it is difficult to accurately predict what the true leakage rate is. It may actually be lower. In the event of implant deflation, saline (the solution of which 70% of our bodies are made) leaks into the surrounding tissues and is absorbed. A relatively brief, simple surgical procedure is required to remove the old implant and replace it with another. In the case of demonstrated saline implant leakage, the implant manufacturers provide a new implant at no charge for the lifetime of the implant and assist with the costs of anesthesia and the operating room for ten years. Dr. Capella’s surgical coordinator will provide more details regarding implant warranties as these have changed over time.
Interference with breastfeeding. Although interference with breastfeeding following breast augmentation is extremely rare, it is possible that the breast gland ducts that empty the breast gland may be divided during breast augmentation and thus interfere with lactation. Additionally, the breasts may be too uncomfortable when engorged, and so lactation may be hindered in this way.
Visible rippling. Individuals with small breasts who have had a large augmentation can be at risk for visible rippling of the overlying skin. This problem is much more common with textured implants and those placed above the pectoralis muscle.